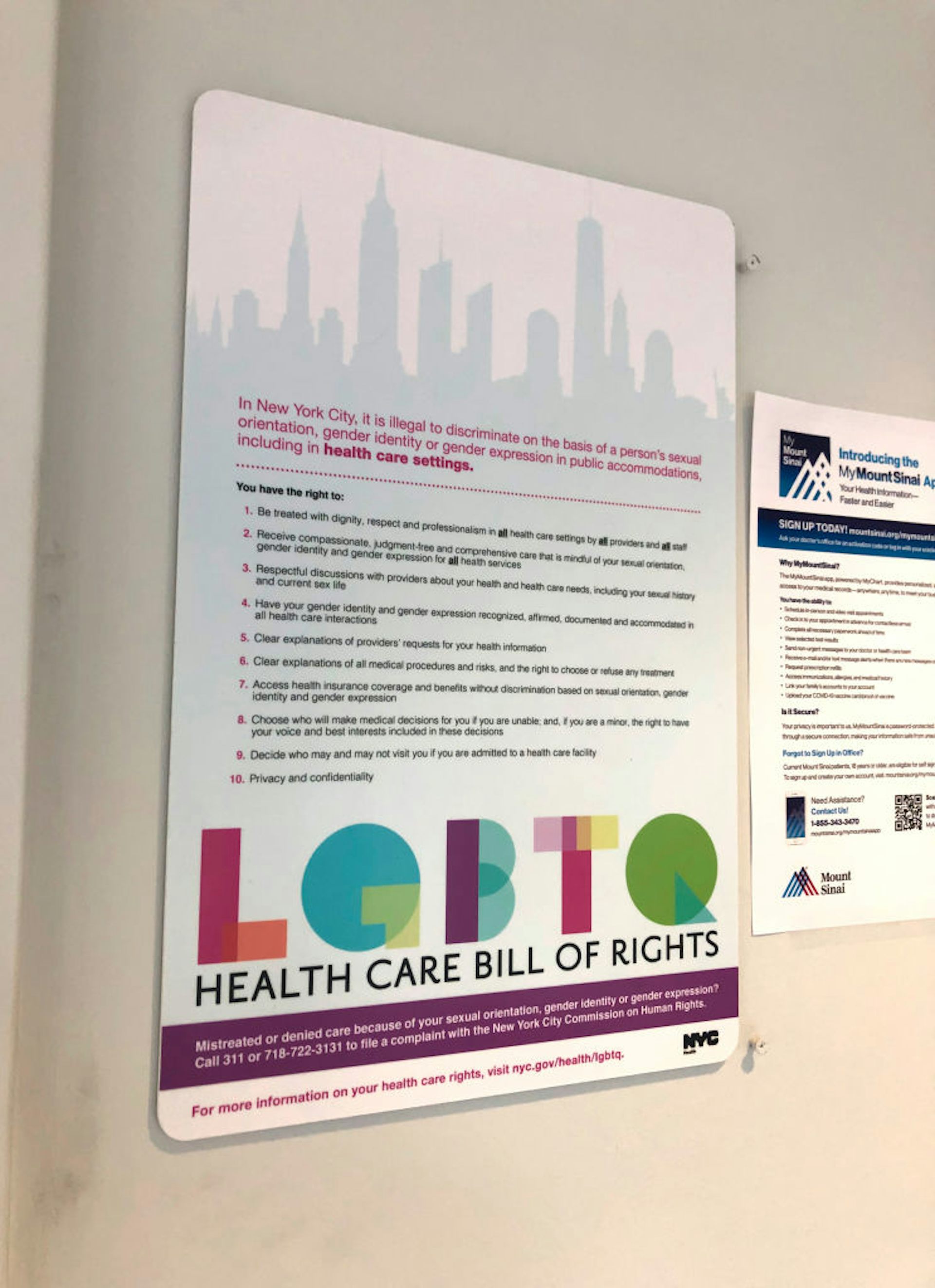
Doctors can refuse to treat LGBTQ+ patients in several states – these religious exemption laws lead to drops in HIV testing
Published in News & Features





An increasing number of U.S. states have passed laws that allow health care providers – including doctors, nurses and pharmacists – to refuse to treat patients based on their personal or religious beliefs. While these conscientious objection laws have long existed for issues such as abortion, their effects on LGBTQ+ people have not been well studied.
As of April 2026, 11 U.S. states have enacted conscientious objection laws specifically targeting LGBTQ+ people. As public health researchers who study the effects of public policies on the health of LGBTQ+ people, we wanted to examine how these laws have affected the roughly 1 in 5 LGBTQ+ Americans living in a state where a provider can legally refuse them care.
Specifically looking at sexual minorities, our research found that lesbian, gay, bisexual and queer adults living in states that passed conscientious objection laws were 28% less likely to report receiving a first-time HIV test, compared to peers in states without conscientious objection laws. These laws did not affect HIV testing rates for heterosexual adults.
Similarly, LGBQ+ adults in affected states were 71% more likely to report being in fair or poor health after the laws passed, compared to those in states without the laws.
We analyzed data from the Centers for Disease Control and Prevention on the health outcomes of more than 109,000 lesbian, gay, bisexual, queer and heterosexual adults from 2016 to 2018. We focused on eight states, comparing two that enacted conscientious objection laws during that period (Illinois and Mississippi) and six that did not (Louisiana, Minnesota, Ohio, Texas, Wisconsin and Virginia).
To isolate the effect of the laws themselves, we compared changes in health outcomes among LGBQ+ and heterosexual adults living in states with or without religious exemptions to health care, both before and after the laws passed. Making all these comparisons at once allowed us to identify differences in health outcomes due to the laws rather than preexisting differences between states.
We found that conscientious objection laws were associated with significant harms to LGBQ+ adults, including a decline in HIV testing and a worsening of self-rated health.
Our findings highlight how laws permitting clinicians to refuse to provide health care to LGBQ+ patients deepen existing health disparities. Notably, conscientious objection laws are just one type of policy restricting LGBTQ+ people’s access to health care.
The Trump administration has slashed budgets for the federal Ryan White HIV/AIDS program and state-level AIDS drugs assistance programs, reducing the availability of HIV prevention and treatment services. States have also moved to restrict access to gender-affirming care for both minors and adults, despite its additional benefit of helping to reduce new HIV infections. Employers have successfully declined to provide insurance coverage of highly effective HIV prevention medications under religious freedom laws.
LGBTQ+ people already face greater health challenges than their heterosexual peers, including higher rates of unmet health care needs and discrimination in medical settings.
HIV preexposure prophylaxis, or PrEP, can lower the risk of contracting HIV from sex by 99%. However, patients are required to receive an HIV test before PrEP can be prescribed. If providers are unwilling or unable to engage with LGBQ+ patients on their sexual health, people who could benefit most from HIV prevention tools, such as PrEP, may never receive them.
Moreover, since the risk of contracting HIV is closely linked to the social determinants of health, such as having safe and stable housing and employment, barriers to HIV testing could further widen health gaps.
Similarly, the worsening in self-rated health among LGBQ+ adults suggests that the cumulative effect of these laws on well-being is real and immediate. A person’s perception of their own health status is one of the strongest predictors of earlier death.
Acknowledging the health consequences of conscientious objection laws could help policymakers and the public better understand their impact.
A 2026 national study found that Americans were more motivated to support policies that address LGBTQ+ inequality when these laws were framed as improving health inequality rather than economic inequality or sense of belonging. This finding suggests that people perceive health inequality as unjust and are less likely to blame LGBTQ+ individuals for those circumstances.
Health care systems can build more affirming environments that actively reassure LGBTQ+ patients will receive fair and equitable care. This can encourage more timely access to preventive services, such as vaccinations and cancer screenings.
For LGBTQ+ people, knowing your rights as a patient and seeking out LGBTQ+-affirming providers and community health centers can help mitigate some of the harms of restrictive laws.
This article is republished from The Conversation, a nonprofit, independent news organization bringing you facts and trustworthy analysis to help you make sense of our complex world. It was written by: Nathaniel M. Tran, University of Illinois Chicago and Periwinkle Seljord-Solberg, University of Illinois Chicago
Read more:
Anti‑LGBTQ+ policies harm the health of not only LGBTQ+ people, but all Americans
Heteronormativity in health care is harmful for LGBTQ+ patients – and a source of tension for queer and trans doctors
Tobacco is still one of the world’s top killers – here are the key obstacles to enacting generational smoking bans
Nathaniel M. Tran received funding from the National Institute on Aging. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health
Periwinkle Seljord-Solberg does not work for, consult, own shares in or receive funding from any company or organization that would benefit from this article, and has disclosed no relevant affiliations beyond their academic appointment.




Comments